Hernia Repair Surgery

Groin Hernia Surgery
What is a Groin Hernia?
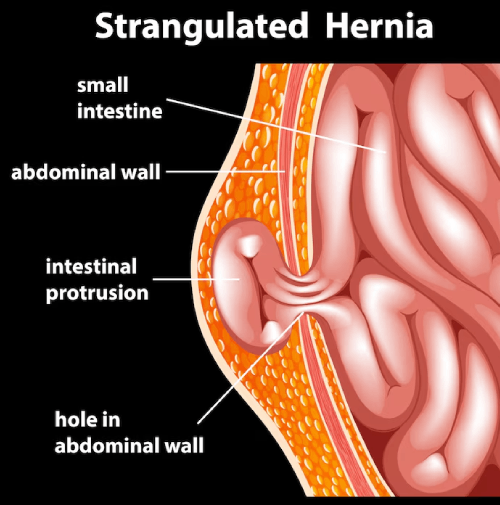
A groin hernia occurs when tissue from inside the abdomen, such as fat or bowel, pushes through a weakness in the lower abdominal wall. This usually presents as a lump in the groin that may be more noticeable when standing, coughing, or straining.
There are two main types:
Femoral hernia – less common, more frequent in women, and associated with a higher risk of complications
Groin hernias do not heal on their own. Over time, they may enlarge and cause increasing discomfort.
Common Symptoms
A visible or palpable lump in the groin
Discomfort or pain when standing, lifting, coughing, or exercising
A dragging or heavy sensation in the groin
In some cases, no pain but a noticeable swelling
If a hernia becomes painful, hard, or cannot be pushed back in, urgent medical assessment is required.
Treatment Options
Surgery is the only definitive treatment for a groin hernia.
Surgical approaches
Open hernia repair
Laparoscopic (keyhole) hernia repair
Both techniques are well established and safe. The choice depends on:
Hernia type and size
Whether it is on one or both sides
Previous surgery
Individual anatomy and medical history
Mesh reinforcement is commonly used as it significantly reduces recurrence rates.
What to Expect from Surgery
Usually performed as a day-case procedure
Operation time is typically 30–45 minutes
Most patients return home the same day
Early mobilisation is encouraged
After surgery
No driving for 2 weeks
No lifting more than 2 kg (a full kettle) for 4 weeks
Return to desk-based work usually within 1–2 weeks
Manual work may require 4–6 weeks
Why Careful Surgical Planning Matters
Groin hernia surgery is common, but outcomes depend on correct technique, appropriate approach, and attention to detail. Individual assessment ensures the safest repair with the lowest risk of recurrence or long-term discomfort.
Ventral Hernia
What is a Ventral Hernia?
A ventral hernia refers to a weakness in the front (anterior) abdominal wall through which tissue protrudes. This term includes hernias that occur away from the groin and are not related to previous surgery.
Common types include:
Umbilical hernia
Epigastric hernia
Other midline abdominal wall hernias
Ventral hernias may be small and painless initially but can increase in size over time.
Symptoms
A lump on the front of the abdomen
Discomfort or pain with movement or lifting
A feeling of pressure or weakness in the abdominal wall
Cosmetic concerns due to visible bulging
Treatment
Surgery is recommended for symptomatic ventral hernias or those that are enlarging.
Repair options
Open repair
Laparoscopic (keyhole) repair
Mesh reinforcement is commonly used, particularly for larger defects, as it reduces the risk of recurrence.
Most ventral hernia repairs are performed as day-case procedures, depending on size and complexity.
Recovery
Same-day discharge in most cases
No driving for 2 weeks
No lifting more than 2 kg for 4 weeks
Gradual return to normal activity
Incisional Hernia
What is an Incisional Hernia?
An incisional hernia develops through a previous surgical scar when the abdominal wall does not heal with full strength. This may occur months or years after abdominal surgery.
Incisional hernias vary widely in size and complexity and often increase over time.
Symptoms
A bulge at or near a previous surgical scar
Discomfort, particularly when standing or lifting
A feeling of weakness in the abdominal wall
In larger hernias, difficulty with movement or posture
Why Incisional Hernias Need Careful Assessment
Incisional hernias do not resolve without surgery. As they enlarge, repair becomes more complex. Early assessment allows:
Proper planning of the repair
Selection of the most appropriate surgical approach
Reduced risk of complications
Treatment Options
Treatment is tailored to the individual and may include:
Open incisional hernia repair
Laparoscopic incisional hernia repair
Mesh reinforcement is standard for most incisional hernias to provide long-term strength.
Smaller hernias may be treated as day case surgery, while larger or more complex repairs may require a short hospital stay.
Recovery
Hospital stay varies depending on hernia size
No driving for 2 weeks
No lifting more than 2 kg for at least 4 weeks
Gradual return to normal activities as advised
Abdominal Wall Hernia (General)
What is an Abdominal Wall Hernia?
An abdominal wall hernia occurs when there is a weakness in the muscles and connective tissues of the abdomen. This allows internal tissue to push outward, creating a bulge.
Abdominal wall hernias include:
Umbilical hernias
Epigastric hernias
Incisional hernias
Spigelian hernias
General Principles of Treatment
Hernias do not heal on their own
Surgery is the only definitive treatment
Timing and technique matter
The goal is a durable repair with minimal disruption to normal life
Patient-Focused Surgical Care
Careful assessment allows:
Accurate diagnosis
Clear explanation of options
Selection of the safest and most appropriate technique
Realistic discussion of recovery and restrictions
This approach supports good outcomes and reduces the risk of recurrence.
After Surgery – Key Advice
Across all abdominal wall hernia repairs:
No driving for 2 weeks
No lifting more than 2 kg for 4 weeks
Gentle walking encouraged
Gradual return to normal activities
These precautions protect the repair and support healing.
When to Seek Medical Advice
You should seek assessment if you notice:
A new or enlarging abdominal or groin lump
Pain associated with a hernia
Changes in the size or firmness of a hernia
Symptoms that affect daily activities
Early assessment allows planned treatment rather than urgent surgery.
Divarication of Recti (Rectus Diastasis)
Patient Information
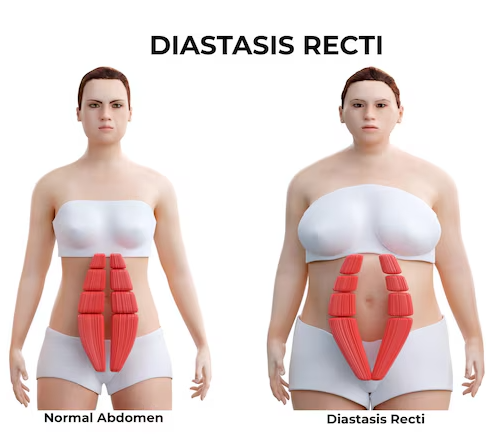
Divarication of recti, also known as rectus diastasis, is a condition where the two vertical muscles at the front of the abdomen (the rectus abdominis muscles) separate along the midline. This separation occurs due to stretching and thinning of the connective tissue (linea alba) between the muscles.
Divarication of recti is not a hernia and does not involve a hole in the abdominal wall. Instead, it represents a loss of tension and support in the midline abdominal tissues.
What Causes Divarication of Recti?
Divarication of recti occurs when prolonged or repeated pressure stretches the abdominal wall.
Common contributing factors include:
Pregnancy (particularly multiple or twin pregnancies)
Significant weight gain or obesity
Previous abdominal surgery
Age-related weakening of connective tissue
Heavy or repetitive straining
Chronic coughing
The condition is common and can affect both men and women.
What Are the Symptoms?
Symptoms vary and may include:
A visible bulge or doming in the midline of the abdomen, especially when standing up or straining
A feeling of weakness in the abdominal wall
Poor core stability
Lower back discomfort
Difficulty performing certain physical activities
Cosmetic concerns related to abdominal contour
Importantly, divarication of recti does not usually cause pain from trapped bowel, unlike a hernia.
Is Divarication of Recti Dangerous?
Divarication of recti is not dangerous and does not carry the same risks as a hernia, such as bowel strangulation or obstruction.
However, it can:
Affect posture and core strength
Contribute to back discomfort
Reduce abdominal wall function
Cause concern due to visible abdominal bulging
In some patients, divarication may coexist with a true hernia, which requires separate assessment.
How Is Divarication of Recti Diagnosed?
Diagnosis is usually made by:
Clinical examination
Observation of abdominal movement during muscle activation
Imaging such as ultrasound or CT scan may be used if:
There is uncertainty about the diagnosis
A hernia is suspected
Surgical planning is required
Treatment Options
Non-Surgical Management (First-Line Treatment)
For most patients, treatment begins with non-surgical measures.
This includes:
Targeted core-strengthening exercises
Physiotherapy focused on deep abdominal muscles
Avoidance of activities that worsen abdominal bulging
Weight optimisation where appropriate
Exercise-based therapy aims to improve function and control, even if the separation itself does not completely close.
When Is Surgery Considered?
Surgery is not routinely required for divarication of recti alone.
Surgical repair may be considered only in selected cases, for example:
Significant functional impairment despite appropriate physiotherapy
Severe abdominal wall weakness
Coexisting abdominal wall hernia requiring repair
Carefully selected patients after full assessment and discussion
Surgery for divarication is not performed to prevent medical complications, but rather to address functional or structural concerns in selected individuals.
Surgical Repair (Selected Cases Only)
When surgery is appropriate, it usually involves:
Re-approximating the rectus muscles
Reinforcing the abdominal wall
Occasionally combining repair with hernia surgery if present
Carefully selected patients after full assessment and discussion
The approach (open or minimally invasive) depends on:
Severity of separation
Presence of hernia
Previous surgery
Individual anatomy
Surgical decisions are made carefully and conservatively.
Recovery and Aftercare (If Surgery Is Performed)
Post-operative recovery varies depending on the procedure performed.
General principles include:
Gradual return to activity
Avoidance of heavy lifting during healing
Structured follow-up
Detailed instructions are provided on an individual basis.
Key Points for Patients
Divarication of recti is not a hernia
It does not carry a risk of bowel strangulation
Physiotherapy is the mainstay of treatment
Surgery is reserved for carefully selected cases
Individual assessment is essential
When Should I Seek Assessment?
You may benefit from specialist review if:
You notice a persistent abdominal bulge
You are unsure whether you have a hernia
You have had previous abdominal surgery
Conservative measures have not helped
A careful assessment allows accurate diagnosis and appropriate advice.
Hernia Surgery – Frequently Asked Questions
Common queries related to the Hernia Surgery.
What is a hernia?
Will a hernia get better on its own?
Is a hernia dangerous?
Do all hernias need surgery?
What types of hernia do you treat?
What are my surgical options?
Will mesh be used?
Is hernia surgery a day-case procedure?
How long does the operation take?
How painful is recovery?
How long is recovery?
When can I drive again?
When can I lift or exercise again?
What are the risks of hernia surgery?
Can a hernia come back after surgery?
What happens if I delay surgery?
How do I know if my lump is a hernia?
Why see a specialist surgeon?
When should I seek urgent medical advice?
Key reassurance for patients
Hernia surgery is common and well established
Most procedures are day-case
Recovery is usually straightforward
Clear advice is provided before and after surgery
Decisions are made based on your symptoms and needs
Reach out to us
If you're experiencing discomfort from a hernia or need advice on hernia repair treatment, don't hesitate to get in touch. Book a consultation with me today to discuss the best treatment options for your condition. Together, we can create a personalised plan to relieve your symptoms and restore your quality of life.
About Us
Consultant-led clinic providing expert surgical care with a focus on patient well-being.
Treatment for
Our Branches
Spire South Bank Hospital:
139 Bath Rd, Worcester, WR5 3YB, UK
©2026 EliteSurgix. All rights reserved