Bariatric Surgery


Bariatric Surgery (Bariatric Metabolic Surgery)
Sleeve Gastrectomy · Roux-en-Y Gastric Bypass · One-Anastomosis Gastric Bypass
Bariatric surgery, also known as metabolic surgery, is an evidence-based treatment for obesity and obesity-related health conditions. It is considered when non-surgical methods such as lifestyle change and medication have not resulted in sustained weight loss or improvement in health.
These operations work by changing how food is processed in the body and by altering gut hormones that influence appetite, fullness, and metabolism.
Why Bariatric Surgery Is Considered
Obesity is a chronic medical condition associated with increased risk of:
Type 2 diabetes
High blood pressure
Sleep apnoea
Heart disease
Fatty liver disease
Joint disease
Reduced quality of life
Bariatric surgery has been shown to result in significant and sustained weight loss, alongside improvement or remission of several obesity-related conditions in appropriately selected patients.
Who May Be Suitable for Bariatric Surgery
Bariatric surgery may be considered for adults who:
Have a BMI ≥40, or
Have a BMI ≥40, or
Have not achieved sustained benefit from non-surgical treatments
Suitability is determined through a structured assessment process, including medical, nutritional, and psychological evaluation.
Considering Ethnicity and Individual Health Risk
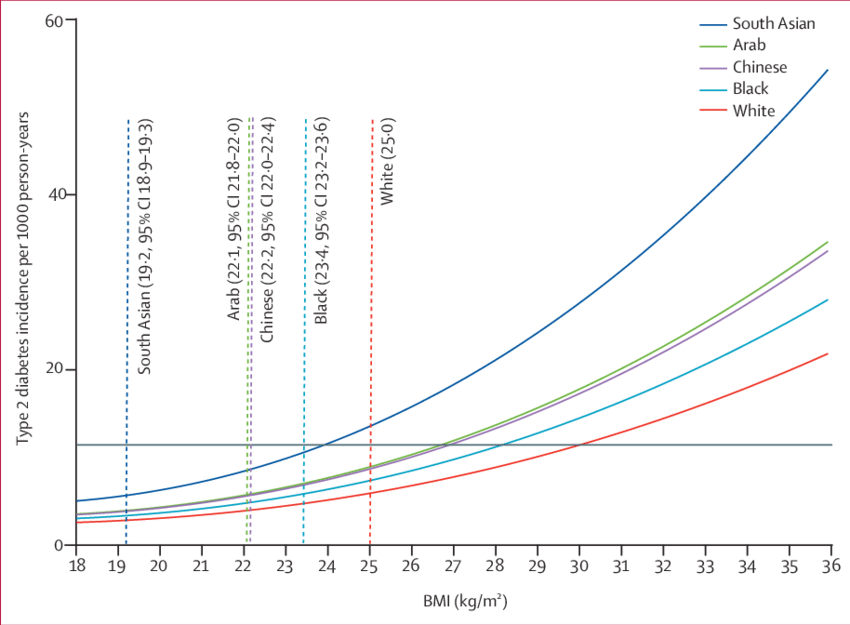
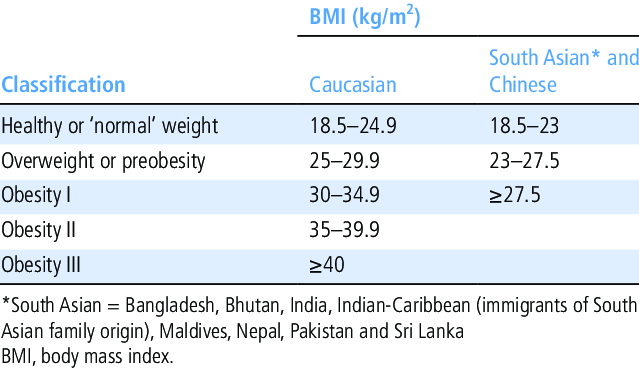
Body mass index (BMI) is a useful screening tool, but it does not reflect health risk equally across all populations. There is strong evidence that people from different ethnic backgrounds may develop obesity-related conditions at lower BMI levels.
People from South Asian, East Asian, Middle Eastern, Arab and some Black ethnic backgrounds are known to develop conditions such as:
Type 2 diabetes
High blood pressure
Fatty liver disease
Cardiovascular disease
at lower BMI values compared with White European populations.
For example:
In South Asian populations, health risks may begin at a BMI of 23–27.5
Type 2 diabetes and metabolic complications may occur at BMI levels below 35
These differences are recognised in UK and international clinical guidance and are taken into account during assessment.
A Personalised, Individualised Assessment
Eligibility for bariatric surgery is not based on BMI alone.
Assessment considers:
Ethnic background and associated metabolic risk
Presence and severity of obesity-related conditions
Pattern and duration of weight gain
Response to previous lifestyle and medical treatments
Reflux or other upper gastrointestinal symptoms
Nutritional, psychological, and overall medical health
This ensures that recommendations are individualised, rather than applying a single threshold or standard pathway to every patient.
Culturally Aware and Inclusive Care
Effective obesity treatment must recognise individual context. This includes:
Cultural and family food practices
Faith-related considerations
Social and work patterns
Practical barriers to lifestyle change
These factors are explored respectfully during consultation, allowing treatment plans to be realistic, culturally sensitive, and aligned with each patient’s values and needs.
Types of Bariatric Surgery
All procedures are usually performed laparoscopically (keyhole surgery).
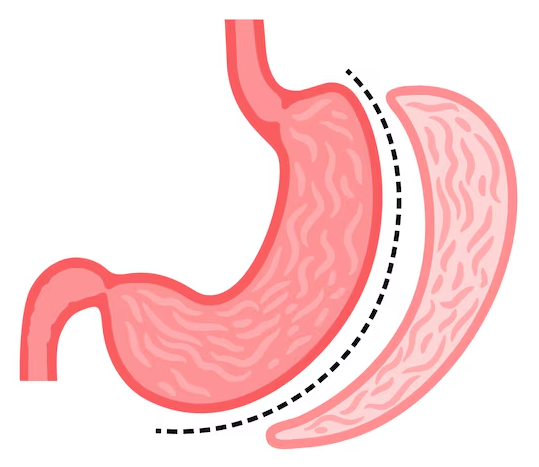
Sleeve Gastrectomy
What is a sleeve gastrectomy?
A sleeve gastrectomy involves removing a large portion of the stomach, leaving a narrow tube-shaped stomach.
How it works
Reduces stomach capacity
Alters gut hormones that regulate appetite
Does not involve bypassing the intestine
Key features
No intestinal bypass
Simpler anatomy compared to bypass procedures
Effective weight loss in many patients
Sleeve gastrectomy is widely performed and well established.
As with other GLP-1–based treatments, side effects are usually gastrointestinal and often improve.
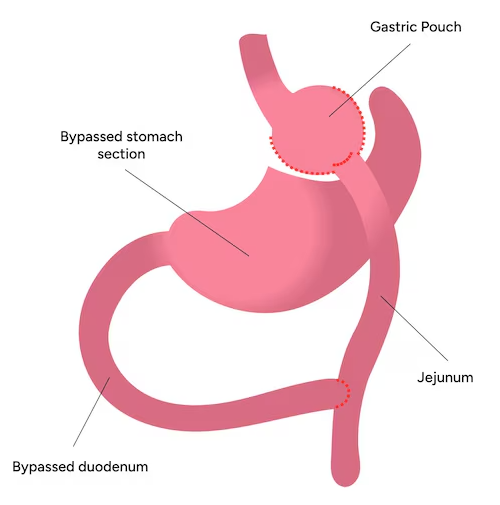
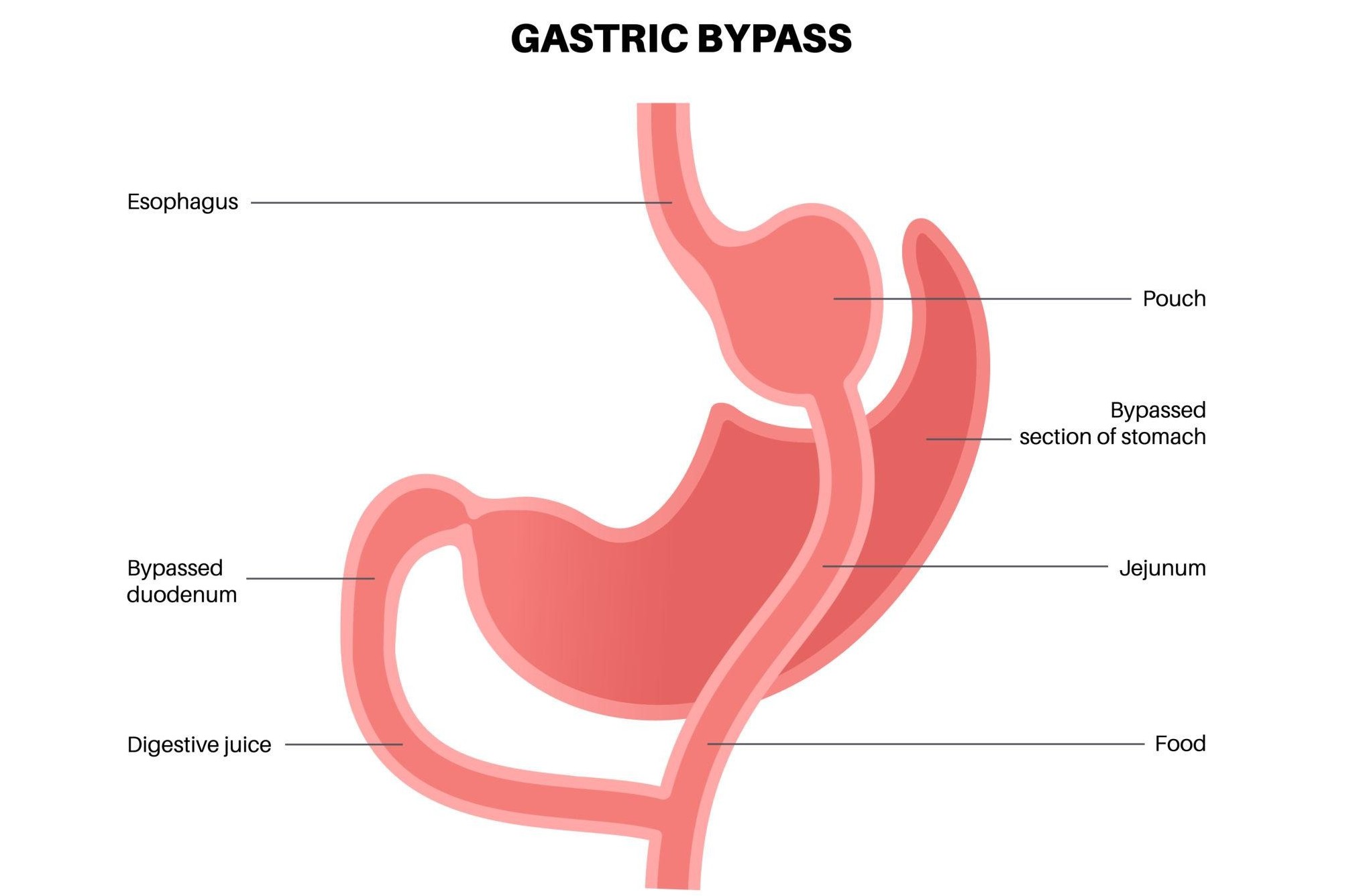
Roux-en-Y Gastric Bypass
What is a Roux-en-Y gastric bypass?
This procedure creates a small stomach pouch and reroutes part of the small intestine, reducing both food intake and nutrient absorption.
How it works
Restricts portion size
Alters gut hormones
Changes nutrient absorption
Key features
Long track record
Particularly effective for type 2 diabetes
Often improves or resolves reflux symptoms
This procedure is considered when metabolic benefit or reflux control is a priority.
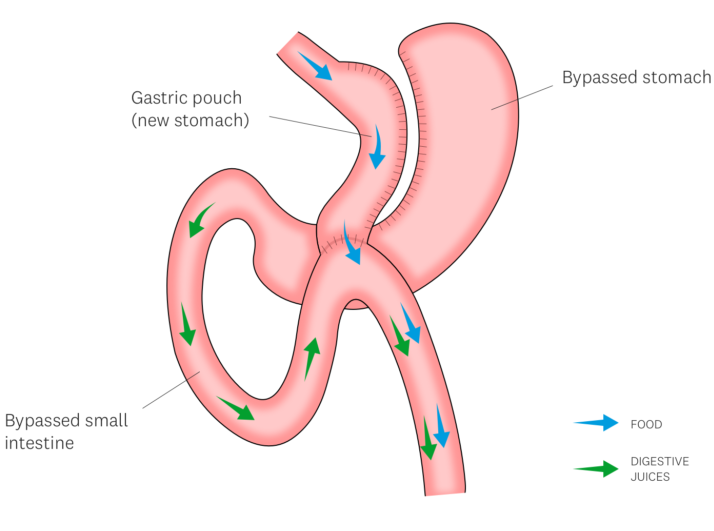
One-Anastomosis Gastric Bypass (OAGB)
What is OAGB?
OAGB involves creating a long narrow stomach pouch and connecting it to the small intestine using a single surgical join.
How it works
Combines restriction with a degree of malabsorption
Produces hormonal changes similar to other bypass procedures
Key features
Single intestinal connection
Effective weight loss in selected patients
Requires careful patient selection and long-term follow-up
This procedure is considered when metabolic benefit or reflux control is a priority.
Expected Outcomes from all three procedures:
Weight loss
Most patients experience substantial weight loss over 12–18 months. The degree varies between individuals and procedures.
Health improvement
Bariatric surgery is associated with improvement or remission of:
Type 2 diabetes
High blood pressure
Sleep apnoea
Fatty liver disease
Joint pain and mobility limitation
Outcomes depend on procedure choice, follow-up, and long term lifestyle change.
Assessment Before Surgery
Before surgery, patients undergo a comprehensive evaluation, which may include:
Medical assessment
Nutritional assessment
Psychological screening where appropriate
Blood tests and imaging
Gastroscopy in selected patients
This process ensures surgery is safe, appropriate, and tailored to the individual.
The Operation and Hospital Stay
Surgery is performed under general anaesthetic
Most procedures take 1–3 hours, depending on type
Typically requires one night in hospital
Early mobilisation is encouraged
This process ensures surgery is safe, appropriate, and tailored to the individual.
Recovery and Aftercare
After discharge
Gradual progression from liquid to solid diet
Regular follow-up with the bariatric team
Lifelong nutritional monitoring
Activity guidance
No driving for 2 weeks
No lifting more than 2 kg (a full kettle) for 4 weeks
Gentle walking encouraged
Gradual return to normal activity
Long-Term Follow-Up
Bariatric surgery requires long-term follow-up to:
Monitor nutrition and vitamin levels
Support weight maintenance
Detect and manage complications early
Vitamin and mineral supplementation is required long term, particularly after bypass procedures.
Risks and Considerations
All surgery carries risks. Bariatric surgery risks may include:
Bleeding or infection
Leak from staple or join sites (uncommon)
Nutritional deficiencies
Internal hernia (bypass procedures)
Weight regain in some patients
These risks are discussed fully during consultation to support informed decision-making.
Important Reassurance
Bariatric surgery is not a “quick fix”
It is one part of a long-term health strategy
Careful assessment and follow-up are essential
Surgery is offered only when benefits outweigh risks
These risks are discussed fully during consultation to support informed decision-making.
Equity & Personalised Care in Bariatric and Metabolic Surgery
Patient Information
Healthcare is most effective when it recognises that people are not all the same. Differences in biology, ethnicity, culture, and lived experience influence how health conditions develop and how treatments work.
In obesity and metabolic disease, there is strong evidence that health risks occur at different body weights in different ethnic groups. For this reason, assessment and treatment should be individualised, rather than based on a single threshold or standard pathway.
Why Equity Matters in Obesity Care
Body Mass Index (BMI) is commonly used to assess weight-related health risk. However, BMI is a screening tool, not a complete measure of health.
Research has consistently shown that people from some ethnic backgrounds develop obesity-related conditions at lower BMI values compared with White European populations.
These conditions include:
Type 2 diabetes
High blood pressure
Fatty liver disease
Cardiovascular disease
Recognising these differences is essential to ensure fair, timely, and appropriate access to care.
Ethnicity and Metabolic Risk
People from the following backgrounds are known to develop metabolic disease at lower BMI levels:
South Asian
East Asian
Middle Eastern / Arab
Some Black ethnic backgrounds
For example:
In South Asian populations, increased health risk may begin at a BMI of 23–27.5, rather than 25–30
Type 2 diabetes may occur at BMI levels below 35, where traditional thresholds might otherwise delay assessment
These differences are recognised in UK and international clinical guidance and are considered during specialist assessment.
What Personalised Care Means in Practice
Personalised care means that decisions are not based on BMI alone.
Assessment may include:
Ethnic background and associated metabolic risk
Presence and severity of obesity-related conditions
Pattern and duration of weight gain
Previous response to lifestyle or medical treatments
Digestive symptoms such as reflux
Nutritional, psychological, and overall medical health
This approach supports equitable decision-making, ensuring patients are assessed according to their individual risk, not a one-size-fits-all model.
Culturally Aware and Inclusive Care
Effective long-term treatment also requires understanding a patient’s context, including:
Cultural food practices
Faith-related considerations
Family and social structures
Work patterns and lifestyle constraints
These factors are discussed openly and respectfully, so that treatment plans are realistic, culturally appropriate, and sustainable.
Key Reassurance for Patients
Lower BMI does not mean lower seriousness
Higher BMI does not mean automatic surgery
Ethnicity-related risk is recognised, not ignored
Ethnicity-related risk is recognised, not ignored
Ethnicity-related risk is recognised, not ignored
Our Commitment
The aim is to provide:
Safe care
Fair access
Evidence-based recommendations
Respect for biological and cultural diversity
Personalised treatment pathways
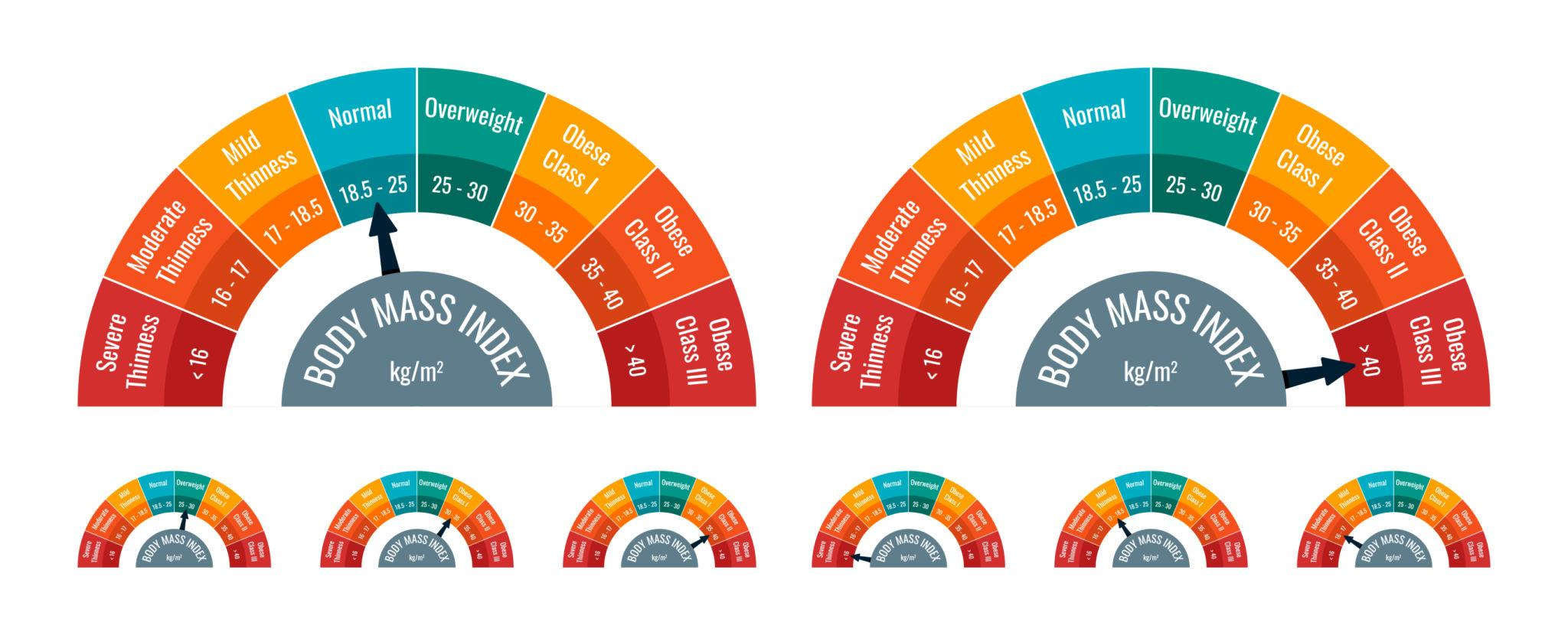
Ethnicity-Adjusted BMI – Explanation
Why BMI Means Different Things for Different People
BMI is calculated using height and weight, but it does not reflect body fat distribution or metabolic risk equally in all ethnic groups.
Some populations develop diabetes and heart disease at lower BMI levels, even when they appear less overweight.
General BMI Categories (White European Populations)
BMI 18.5–24.9 → Lower risk
BMI 25–29.9 → Increased risk
BMI ≥30 → Obesity
BMI ≥35 with health conditions → Consideration for specialist treatment
Adjusted Risk Awareness (Selected Ethnic Groups)
For people from South Asian, East Asian, Middle Eastern, Arab and some Black backgrounds:
Health risks may begin at BMI 23–27.5
Type 2 diabetes may occur at lower BMI levels
Metabolic disease can develop earlier
This does not mean automatic treatment — it means earlier assessment when medical risk is present.
What This Means for You
BMI is interpreted in context, not in isolation
Ethnicity is one of several factors considered
Health impact matters more than a number alone
Assessment focuses on risk, not labels
Important Message
There is no single BMI threshold that applies to everyone.
Personalised assessment allows fairer, safer, and more effective care.
Reference or Sources
Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies - PubMed
BMI: preventing ill health and premature death in black, Asian and other minority ethnic groups | Guidance | NICE
https://research.sahmri.org.au/en/publications/appropriate-body-mass-index-for-asian-populations-and-its-implica/
Identifying and assessing overweight, obesity and central adiposity | Overweight and obesity management | Guidance | NICE?
https://www.japscjournal.com/articles/obesity-asia-pacific-region-current-perspectives?language_content_entity=en&
Bariatric Surgery and Cardiovascular Risk
Obesity and Cardiovascular Disease
Obesity contributes to:
Hypertension
Dyslipidaemia
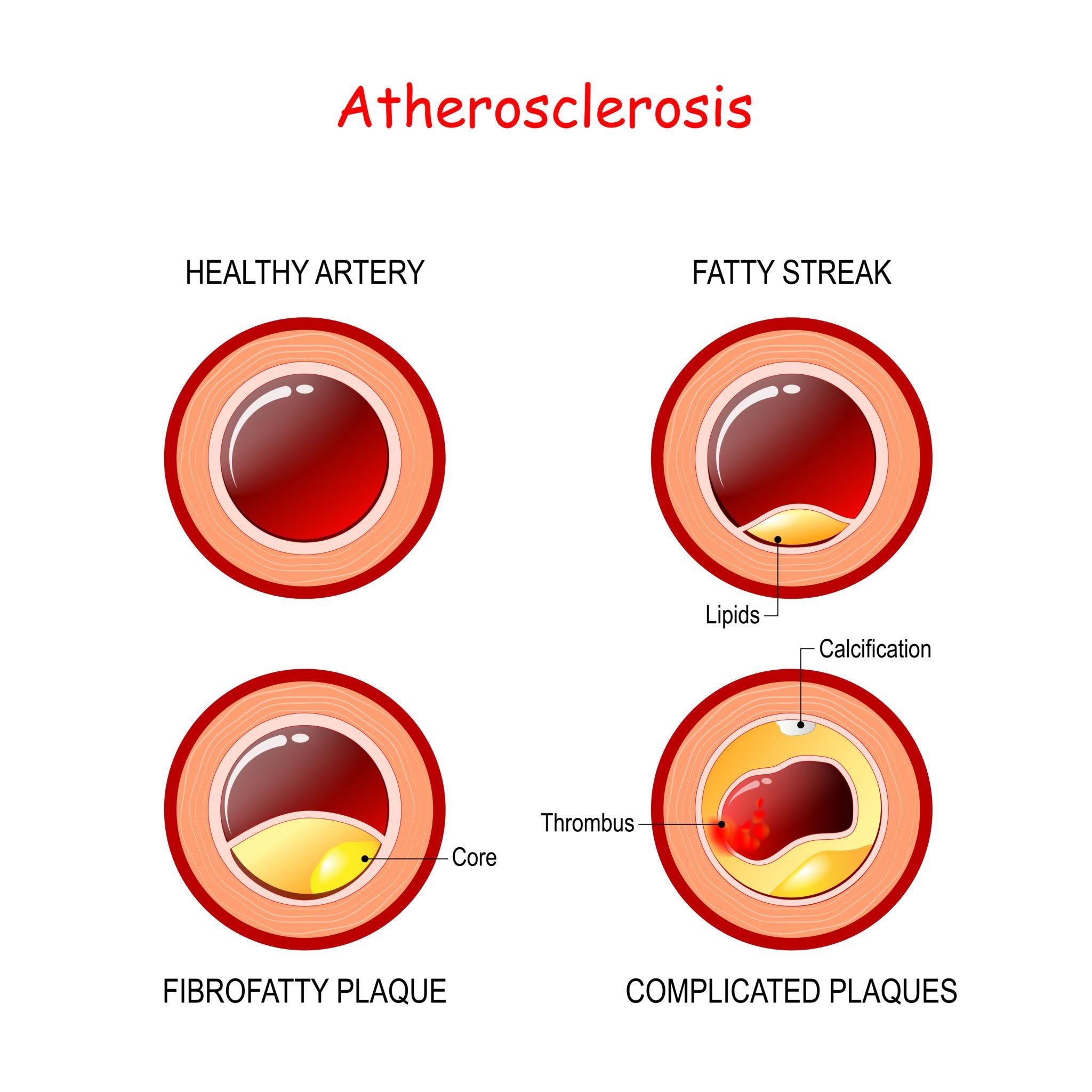
Atherosclerosis
Evidence
Long-term observational studies show:
Reduction in cardiovascular events
Reduction in overall mortality
Improvement in metabolic markers
Bariatric Surgery for Type 2 Diabetes
Why Diabetes and Obesity Are Linked
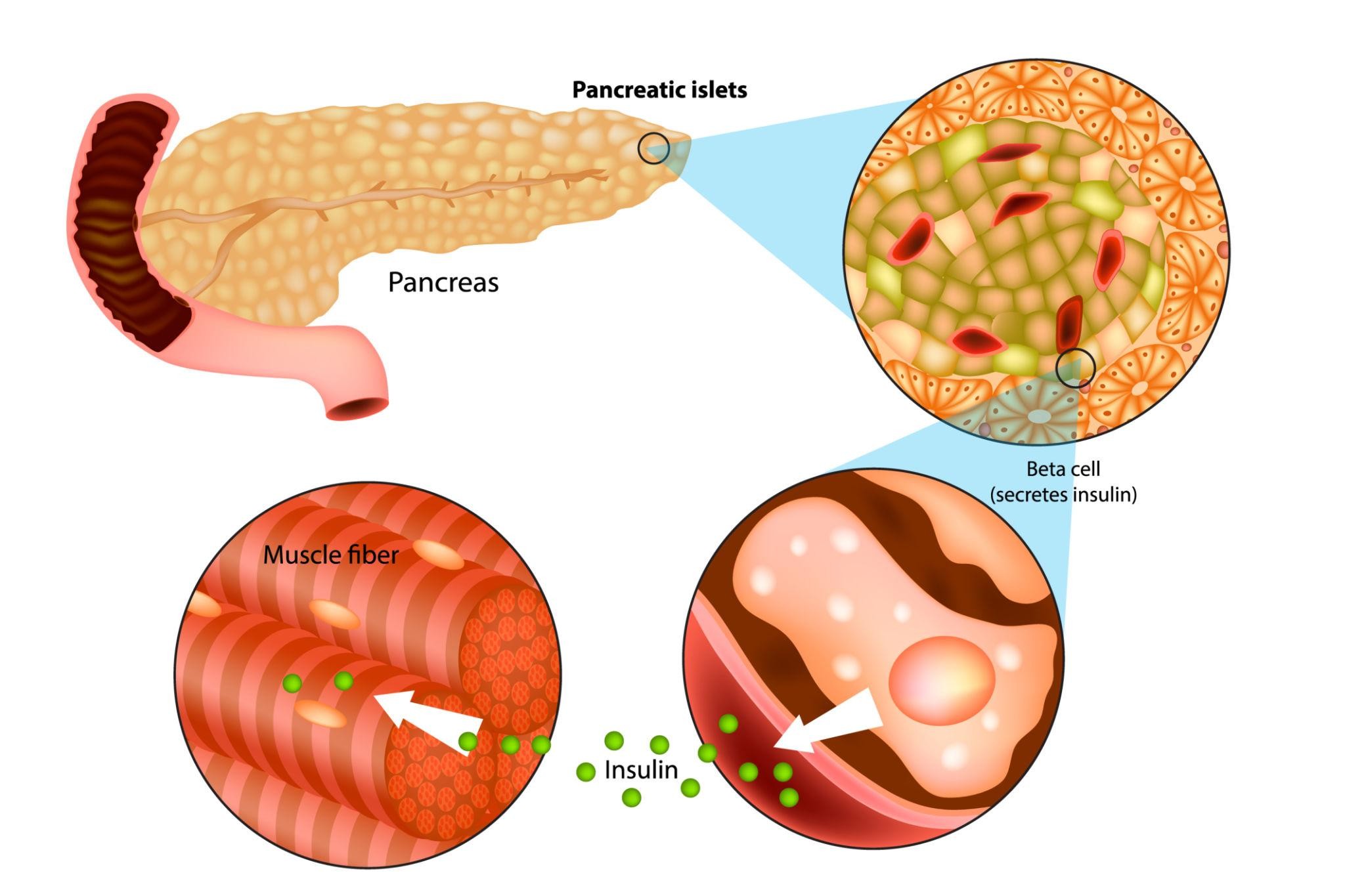
Excess visceral fat contributes to:
Insulin resistance
Increased pancreatic workload
Progressive beta-cell dysfunction
Metabolic surgery alters gut hormones and improves insulin sensitivity.
What Evidence Shows
Randomised trials demonstrate:
Greater improvement in HbA1c compared with medical therapy alone
Higher rates of diabetes remission
Reduced medication dependence
Early intervention (shorter diabetes duration) is associated with higher remission rates.
Bariatric Surgery for Obstructive Sleep Apnoea
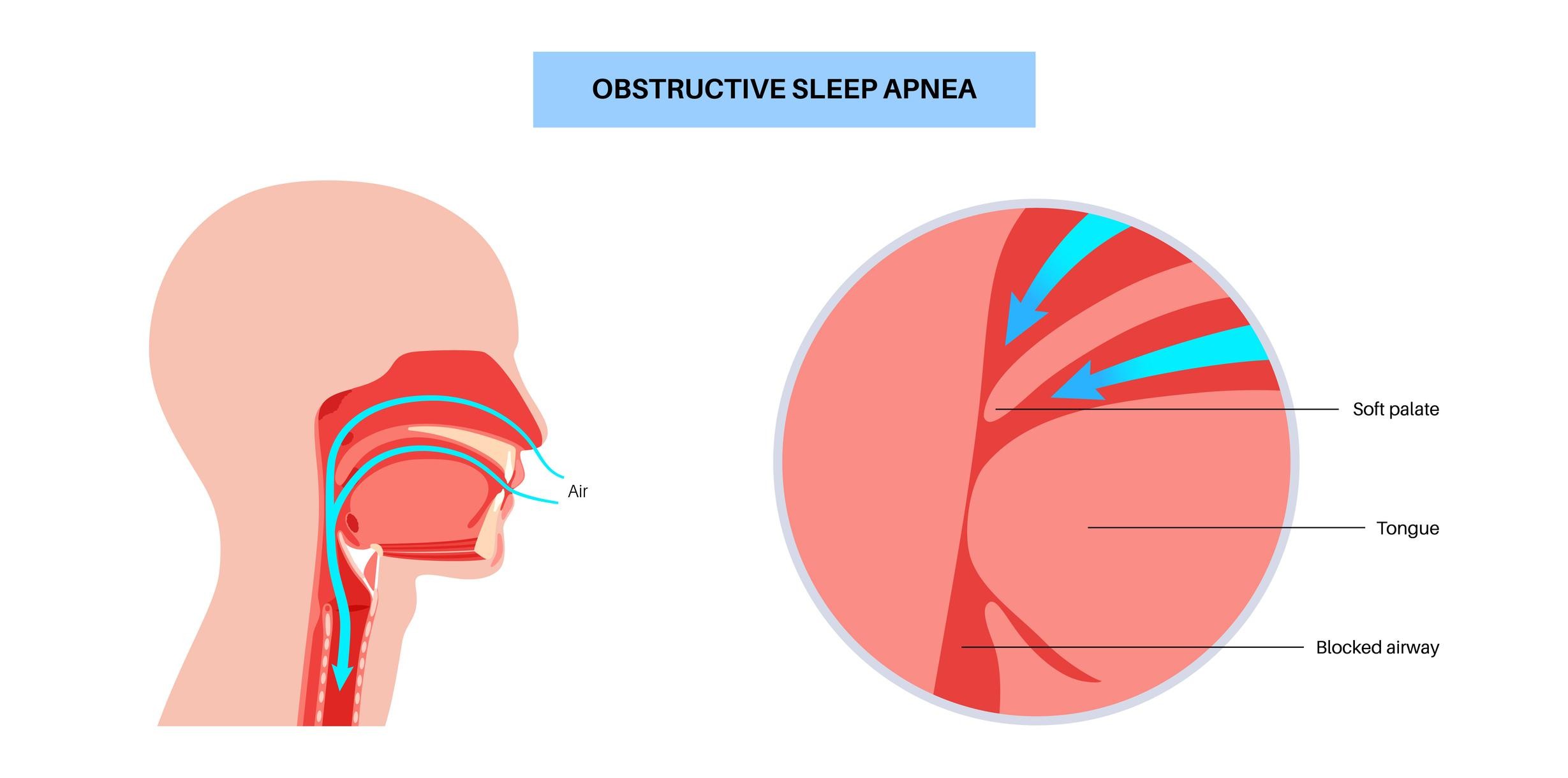
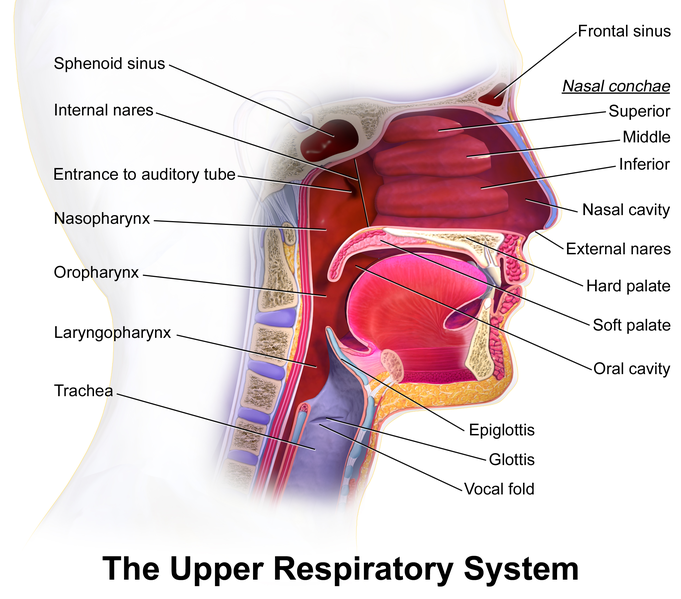
Why OSA Occurs
Excess neck and visceral fat narrows the upper airway, increasing collapse during sleep.
Evidence
Weight reduction is associated with:
Reduced apnoea-hypopnoea index
Reduced CPAP requirements
Improved daytime function
Surgery may be considered in moderate to severe OSA linked to obesity.
Bariatric Surgery for Osteoarthritis & Joint Pain
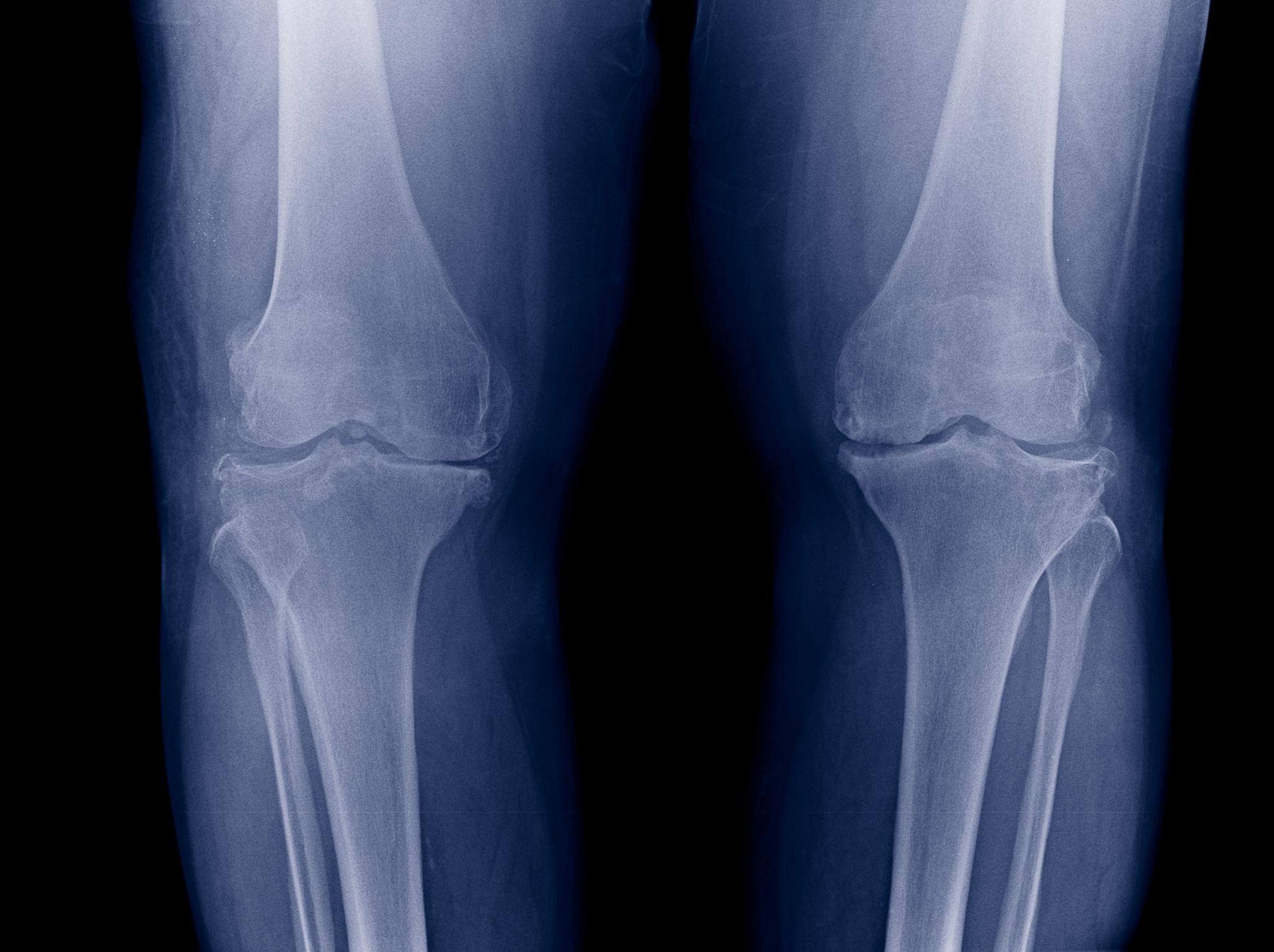
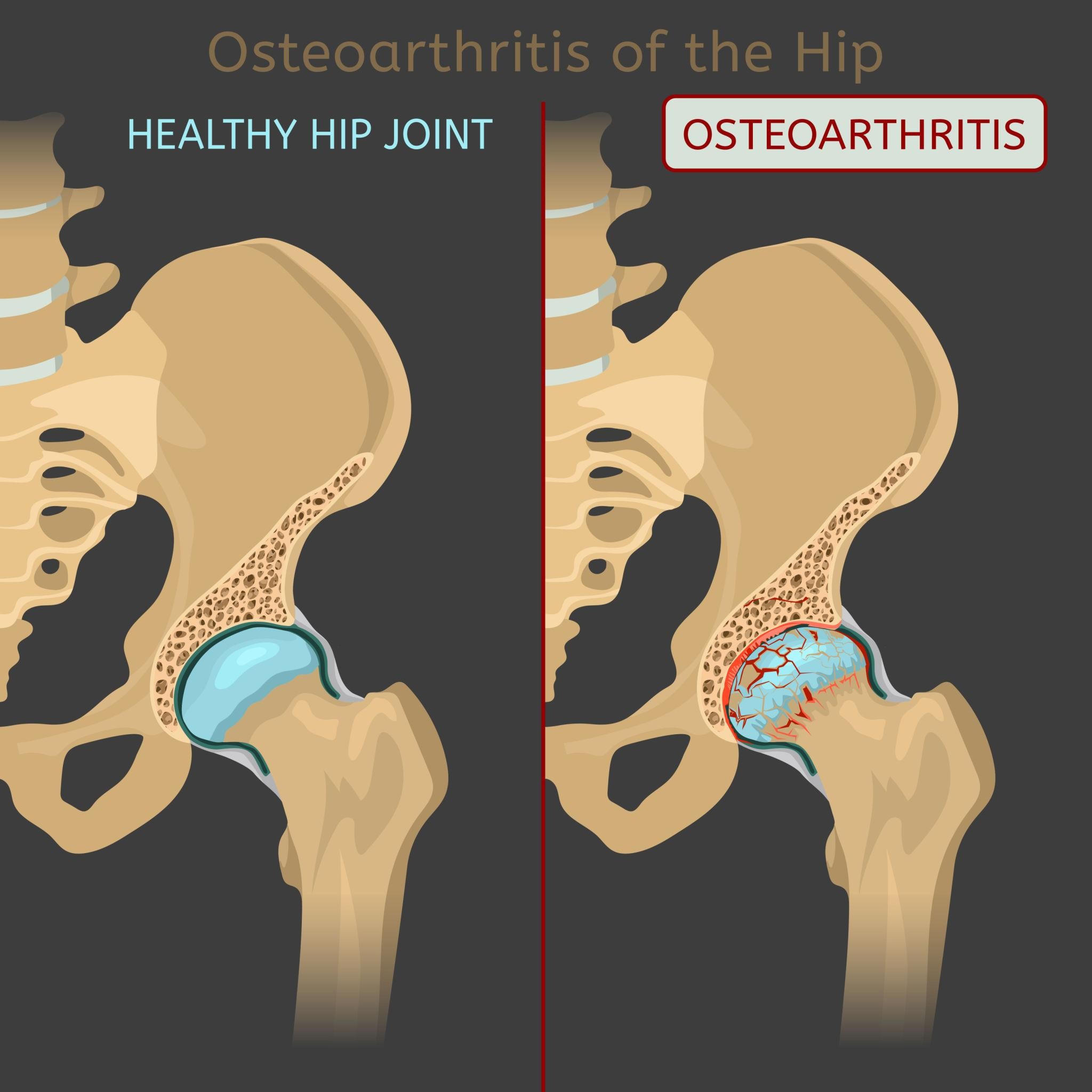

Mechanical Load and Joint Degeneration
Every 1kg of body weight increases knee load several times during walking.
Evidence
Weight reduction is associated with:
Reduced knee pain
Improved mobility
Slower osteoarthritis progression
Surgery may support patients struggling with mobility due to weight.
Weight Loss Before Joint Replacement
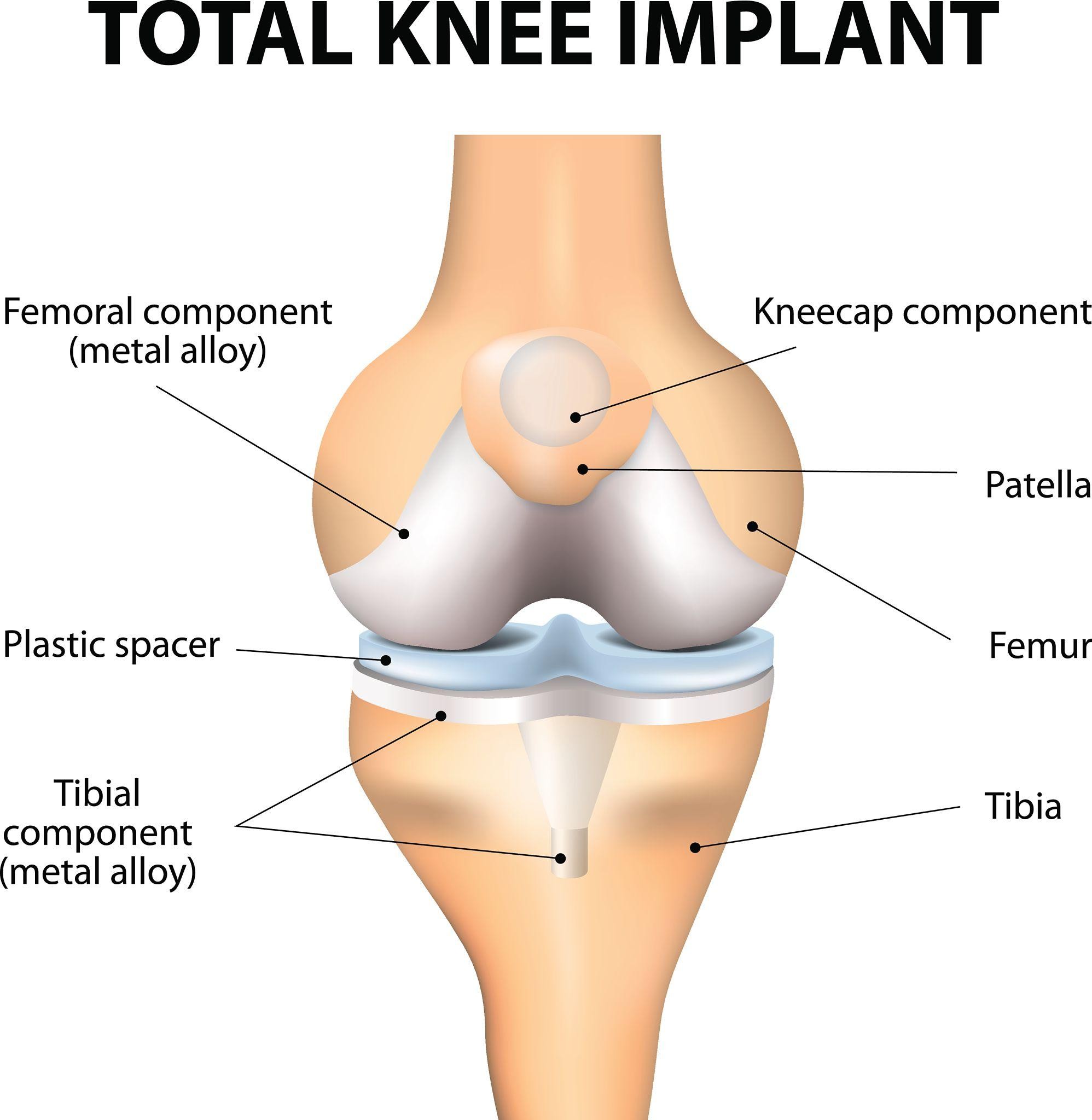

Higher BMI is associated with:
Reduced knee pain Increased surgical risk
Higher wound complication rates
Longer recovery
Weight reduction may:
Reduce operative risk
Improve rehabilitation outcomes
Bariatric Surgery and Fertility
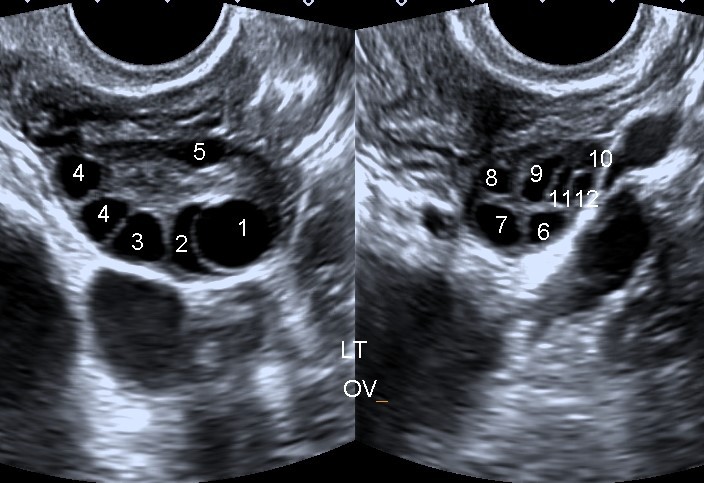
Obesity and Reproductive Health
Obesity may contribute to:
Irregular ovulation
PCOS
Reduced fertility
Pregnancy complications
Evidence
Weight reduction is associated with:
Improved ovulatory function
Improved metabolic profile
Reduced gestational diabetes risk
Pregnancy is usually deferred 12–18 months after surgery.
Bariatric Surgery and Fatty Liver Disease
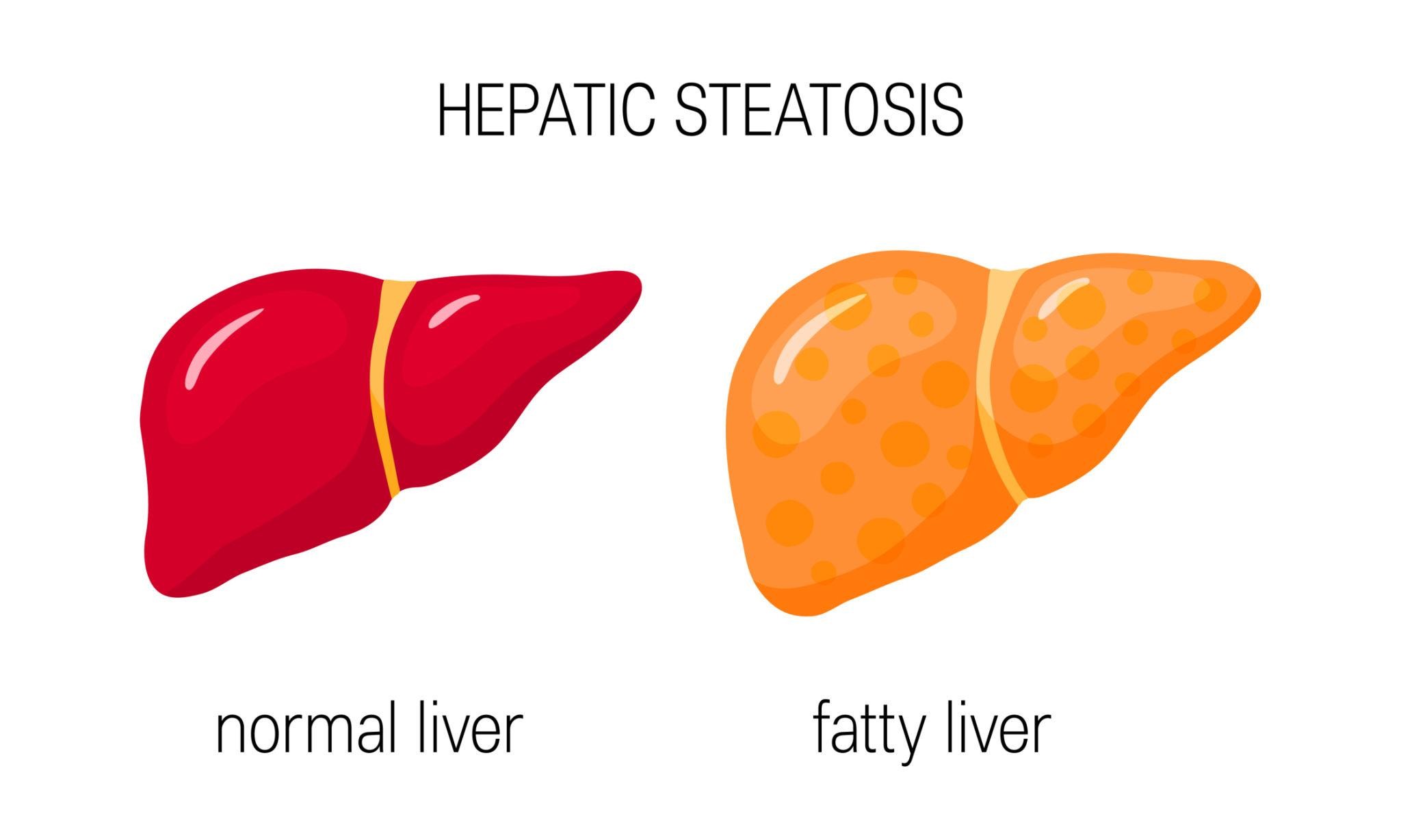
Why It Matters
NAFLD is closely linked to obesity and insulin resistance.
Evidence
Weight reduction is associated with:
Reduction in liver fat
Improvement in inflammation
Improvement in fibrosis markers in some patients
Bariatric Surgery – Frequently Asked Questions
Common queries related to the Bariatric Surgery.
Is bariatric surgery safe?
Which operation is best for me?
How much weight will I lose?
Will I need to take vitamins?
Can bariatric surgery improve diabetes?
Is bariatric surgery reversible?
Will I regain weight?
How long before I can return to work?
When should I consider specialist assessment?
Key Message for Patients
Bariatric surgery is an evidence-based treatment
Careful assessment is essential
Procedure choice is individualised
Long-term follow-up matters
Informed decisions lead to better outcomes
Contact Us for Bariatric Surgery Consultation
If you’re considering bariatric surgery as a weight loss solution, it’s important to have a thorough consultation with a specialist to discuss your options and create a tailored plan. Contact us today to book an appointment or to find out more about our bariatric surgery services.
About Us
Consultant-led clinic providing expert surgical care with a focus on patient well-being.
Treatment for
Our Branches
Spire South Bank Hospital:
139 Bath Rd, Worcester, WR5 3YB, UK
©2026 EliteSurgix. All rights reserved
Frequently asked questions
Queries related to the features, functionality, pricing, and availability of a product or service.
How fast will I receive my designs?
Why don’t we just hire our own in-house designer?
How big/complicated can my Webflow site be?
Do I get any revisions?
How do I request designs?